Site Menu:
| This is an archived Horseadvice.com Discussion. The parent article and menus are available on the navigation menu below: |
| HorseAdvice.com » Diseases of Horses » Skin Diseases, Wounds, and Swellings » Swellings / Localized Infection / Abscesses » Diagnosing and Assessing Swellings in Horses » |
| Discussion on HELP!! PREGNANT MARE WITH ABCESSED MANDIBLE | |
| Author | Message |
| Member: mitma |
Posted on Monday, Mar 26, 2007 - 4:36 pm: Dear HA colleagues and Dr. O,Well, last Friday, my three "ex-PMU" mares arrived from Canada... not in perfect shape, of course, but, not dying either. However, 24 hours after their arrival, I noticed some swelling on the lower aspect of one mare's jaw, specifically, the straight portion of her left mandible about half way between her lower lip and masseter muscle areas. There also appeared to be two purulent tracts that were draining. Fortunately, this is one of the mares that has a sweet disposition and had allowed me to catch and lead her. Well, I thought this was not the usual place for strangles, and though it was Saturday night, I called my vet and he came out. He agreed that it was not likely strangles, but we cultured it anyway. In order to clean/irrigate the area, we had to sedate her and once she was "calm", he irrigated about 50-75 ccs of pus from the wound. He took some skull xrays of the area and suggested I start some antibiotics; though, I'm comfortable giving injections, we decided to start with oral Bactrim DS BID until the culture/sensitivities come back. Well, today he called to say that the xrays show a definitive mandibular abscess which does NOT appear to be dental in origin. We assume that she sustained a penetrating injury in the last few/several weeks that has produced this ???osteomyelitis of her mandible. Now, here's the big question: MEDICAL VS. SURGICAL TREATMENT???? And, does her pregnancy and/or her gestational age (still a big, big guess, of course, but for the past three years, she has always foaled in early to mid May... last year she was loose in the pasture with the stallion from May 15th until late November, but I'm still betting that she was bred during her foal heat). What is really the best course of therapy for this mare and what risk does that, or the lack of any therapy, expose her unborn foal to???? Thanks in advance for any thoughts! Martha 
|
| Member: corinne |
Posted on Monday, Mar 26, 2007 - 7:08 pm: Gosh! Just sending well wishes her way until Dr. O writes back. What a beautiful mare and what a wonderful person you are rescuing them! |
| Member: zarr |
Posted on Monday, Mar 26, 2007 - 7:53 pm: So sorry Martha, poor girl she looks very nice. Only experience I've had was a friends mare got kicked it the lower jaw and it splintered and became abcessed. The vet just had us keep it clean and medicated. I pulled out 2 small bone splinters and thought more should have been done but not my mare. She did finally get well??!! Dr. O will have good ideas. All the best Cindy |
| Moderator: DrO |
Posted on Tuesday, Mar 27, 2007 - 7:59 am: Martha, the decision to do surgery are best made from the findings on the radiograph: does the veterinarian feel there are areas of bone that are so compromised they should come out?DrO |
| Member: mitma |
Posted on Tuesday, Mar 27, 2007 - 9:22 am: Thanks for everyones' concerns and comments... Well, right now we are getting ready to load in the trailer and take a ride to our local (large) equine practice that has just recruited an equine surgeon from VA Tech. Basically, my beloved ambulatory vet told me he didn't think he could do more (surgically) in the field and I assume that was based his interpretation of the xrays (so, Dr. O, I don't yet know the answer to your question); the xrays were, of course, take with a portable, hand-held machine, so perhaps they are less than ideal. Basically, when we get to the clinic today, we'll get an exam, some additional xrays I suspect, and then some sedation to explore and I/D the wound further; when I spoke with the clinic last night they also mentioned the need to determine whether there is any communication of the wound with the oropharynx (I may have forgotten to mention that on Saturday when my local vet was irrigating the wound, the mare started "chewing" as if something was getting in her mouth...) So, more to come...Martha |
| Moderator: DrO |
Posted on Tuesday, Mar 27, 2007 - 4:51 pm: With sedation so the horse lowers his head and holds still, this is a pretty easy place to get good field radiographs so I would not think this a limit in the interpretation. Usually obliquing the shot (the machine is held dorsal to the mandible and pointing down at about a 30 degree angle) so the mandible does not overlie the other side provides a pretty clear though slightly magnified view because the cassette cannot be put up right against the side with the lesion.DrO |
| Member: mitma |
Posted on Wednesday, Mar 28, 2007 - 5:08 pm: O.k... Most physicians have been taught the expression "when you hear hoofbeats, think horses, not zebras" and that appears to be true in veterinary medicine also! Here's the update... (BTW, Dr. O, my vet did take obliques in the field on Saturday evening) My mare has an "osteolytic lesion of the left hemimandible" which, based on the contrast fistulagram performed, originates from her 3rd premolar. At the large equine clinic we visited yesterday she was sedated again, with detomidine, then butorphanol, got the additional xrays and contrast fistulagram, then got an incredible exam of the oropharynx with the hopes of extracting the 3rd premolar. Sadly, we discovered that the tooth was fractured down to almost the gumline and the surgeon was unable to extract it in the normal fashion. He feels that a general anesthetic is the only reasonable approach now in order for the tooth remnant to be removed via an intraoral route, or even possibly through a mandibular incision. He also thinks that it is likely she's had this for "years" and that we can wait for any further therapy. He thought that the possibility of hypoxia during a GA would put the foal at unnecessary risk, given the chronicity of this problem with the mare. So, she should foal in the next month or so, then after 60 to 90 days we'll go in for the definitive surgery later in the summer. Meanwhile, she's still on antibiotics and I should hear about the culture later today, though I know it's likely to be "mouth flora". I'll keep everyone posted... Thanks!Martha |
| Moderator: DrO |
Posted on Thursday, Mar 29, 2007 - 6:54 am: But if your patients are a herd of zebras...Thanks for the update Martha, The fractured tooth prevents him from being able to put strong traction on it, necessitating the use of tools that require general. That all makes sense. What antibiotic and dosage are you using? Would it be possible to post the radiograph and fistula-gram? DrO |
| Member: mitma |
Posted on Friday, Mar 30, 2007 - 12:02 am: Dr. O,She's currently on TMP/Sulfamethoxazole (Bactrim DS), 10 tabs BID; this is day 5 of therapy and we're trying to get 10 - 14 days of antibiotics into her. Each day is NO easier "tricking" her into eating her grain in less than one to two hours. Since she is pregnant and was "underfed" at the ex-PMU ranch, I would think she would gobble up her grain, but maybe the antibiotic is really an awful tasting to her, or maybe she's just not used to grain. I've tried molasses, applesauce, baby food in apple/banana and carrot flavors, and combinations of these items. Nothing has worked well... she really doesn't seem to like any added stickiness in her feed. I am most successful if I dissolve the Bactrim in a very small amount of water and mix it into her feed and hope that she hasn't eaten abundant hay just prior. Anyway, my vet called me today and said that the preliminary culture is growing a Group C Strep... final identification is still pending, but fortunately, it is sensitive to the Bactrim. Regarding the xrays and fistulagram, I've asked the clinic to email them to me and I will post them when I get them. Thanks! Martha |
| Member: shirl |
Posted on Friday, Mar 30, 2007 - 12:28 am: Martha, have you tried grinding up the tabs in an old coffee grinder, putting the powdery stuff in bran and then wetting the whole bit? Try it. My horse wolfs down meds that way.Good luck, Shirl |
| Member: freshman |
Posted on Friday, Mar 30, 2007 - 1:00 am: I'm not clear on how you are administering the medications, but I think it sounds like you are putting them on/in her feed? A much more direct route is oral administration via a large syringe, in the same fashion that you would give a paste dewormer.Ask your vet for a 60cc syringe, cut off the tip, and put the ground medications in with a mix of coke, pancake syrup, or anything else. Warm water will work, but most horses appreciate the addition of something to cover up the taste of the meds, and using something like the molasses, etc, will make most horses easier to deal with in the long run. Even so, giving oral meds in this fashion will make some horses very ornery. Unfortunately, these are usually also the horses that won't eat them with their feed. Something has to give, so it may be necessary to use a chain over the horse's nose, or have some help to get the meds into her. Good luck with this mare! She is very lucky to have found her way to your home, and I hope she does well and gives you a nice foal. These 'unemployed' horses need every kindness that comes their way. |
| Moderator: DrO |
Posted on Friday, Mar 30, 2007 - 7:10 am: Hello Martha,Two points. There is controversy whether the antibiotic sensitivity test of potentiated sulfas is accurate with respect to Strep, especially in a purulent (puss) environment. In-vitro sensitivity has not always translated to in-vivo efficacy. You may find more about this on the insert that comes in the bottle. Having started you can judge by clinical response. Second is prolonged use of potentiated sulfas has resulted in birth defects in foals for more on this see, Treatments and Medications for Horses » Antibiotics and Antimicrobials » Trimethoprim -Sulfa. DrO |
| Member: erika |
Posted on Friday, Mar 30, 2007 - 9:12 am: Dr. O, just curious why this horse wouldn't be on injectable penicillin? I thought it was the drug of choice for strep. Is it because of the pregnancy? Sorry if I missed something... |
| Member: dawson |
Posted on Friday, Mar 30, 2007 - 6:36 pm: Hey Shirley I'd grind and mix or crush and syringe too. But.... on the lighter side. Coke?Man, I know what that stuff did to my teeth when I drank it for a month...3 cavities. Poor girl has a bad tooth already. Martha, Thanks for all the detailed information on what's been happening, I have not had to come up across this type of issue before, your information is much appreciated. |
| Member: shirl |
Posted on Saturday, Mar 31, 2007 - 12:46 am: Hi Dawson,T'wasn't me that mentioned "Coke"! I suggested using bran with the ground up meds. Coke sounds interesting to say the least. Cheers, Shirl |
| Member: mitma |
Posted on Saturday, Mar 31, 2007 - 1:32 am: Whew! Thanks everyone for all the thoughts and comments...So, first of all I will try to now upload the films for all to view... if I'm not successful, I'll work on it again tomorrow. Regarding the antibiotic issue... Erika, my vet did offer me the option of IM penicillin every 12 hours and I am quite comfortable giving all sorts of injections (at least to humans), however, he told me that the volume of drug to administer would be like 30 ccs or so (alot to inject IM... in my mind) and that it would be best to give the drug in the "rear", i.e, the semimembranosis and semitendonosis muscles, which are somewhat low on the hind end; since this mare is new to me and not well socialized/trained, I was concerned that this type of injection might turn out badly. Also, I really don't have any help now, so everything I do to her, I'm doing alone (not ideal, but it is what it is for now). Dr. O, your comments on in vitro sensitivity vs. in vivo "results" of sulfa antibiotics are quite interesting... perhaps, that explains the opposing opinions I got from my local equine vet and the equine surgeon; my vet thought we should try to complete a course of therapy, but the surgeon didn't feel it would help. I will say this, however, I think this mare feels much better now. She is much more energetic and interactive now (and I think that is part of the difficulty I'm experiencing with giving her oral antibiotics, because she's able to effectively protest now). I realize there may be many factors involved... she's finally settling in to her new home, getting regular, excellent nutrition, attention, etc... plus, the submandibular wound has been opened/drained twice. On the other hand, I can't exclude that the antibiotics may be helping and though I am NOT someone who wants to see antibiotics given for just any "infectious" reason (they are certainly over prescribed to us humans!), I would really like to finish a reasonable "therapeutic" course of 10 to 14 days. Now, that being said, the issue of foal birth defects is troubling, but do you really think 10 - 14 days would be considered "prolonged" therapy?? This mare is in her 10th month of gestation, so aren't we done with organogenesis (which I presume is when most birth "defects" occur) and shouldn't the foal be somewhat "tolerant" of maternal medical therapies now??? I will look at your article on sulfas... For Shirley, Kristin, and Dawson... thanks for your comments. The last two feedings have proceeded relatively well; in that, she has eaten most of her grain in under 45 minutes! FYI, I tried early on to administer the drug orally via a catheter tip syringe (filled with a yummy molasses/applesauce base and the ground up Bactrim DS), but I almost "got killed"; needless to say, she is VERY sensitive about her mouth... probably because it hurts alot, in addition to the fact that she's not been well trained (most of these ex-PMU mares from really large operations apparently received all of their medical care while held in a chute); when I quietly attempted the syringe maneuver, she reared straight up and lunged forward flinging me a bit... oh well! For now, I am reluctant to use a twitch... (that's probably for another thread) and though I know there's the "it generates endorphins/enkelphins" theory, I also think it might disrupt the trust I think I'm developing with this mare... given, that we still have to get through foaling, etc.., I would really like to keep our relationship moving in a positive direction. More updates later... Thanks! Martha |
| Member: mitma |
Posted on Saturday, Mar 31, 2007 - 2:23 am: O.k., I've been trying for more than an hour to reduce the size of the xrays in order to upload them, as they are all more than 64kb... Clearly, I do not understand how to edit picture files. I will keep working on it in the next few days after I talk to my computer whiz brother-in-law.Martha |
| Member: terrilyn |
Posted on Saturday, Mar 31, 2007 - 6:33 pm: Oh dear, Martha...just picked up your phone message this morning so I went looking for the thread--not one that I had been following. All I can say is, thank goodness the mare didn't throw you through the wall! I'm glad you're ok, and very sorry that you're dealing with a problem of this magnitude so shortly after your horses' arrival! Will look for the xrays to load. This is extremely interesting...not a problem you read about every day. Just sorry it's happening to you! Will talk to you soon...take care, and BE CAREFUL. |
| Moderator: DrO |
Posted on Saturday, Mar 31, 2007 - 7:24 pm: While both of your points are worth consideration I am not sure they abrogate the problem. Most of the birth defects have occurred with mares being treated for EPM so were on longer courses than 14 days but bone infections often require prolonged therapy.Second the lesions were not so much lack of organogenesis but those of necrosis and degeneration secondary to vitamin deficiency so I am not sure late pregnancy is protective. If the mare can graze fresh green grass which is rich in the active form of folate would probably be protective but current recommendations suggest monitoring pregnant mares on potentiated sulfas. DrO |
| Member: mitma |
Posted on Sunday, Apr 1, 2007 - 3:22 pm: Terri,Thanks for your concern... but, remember, this all started several months ago as "my midlife crisis", so, I am actually having a very meaningful and rewarding experience and I am trying not to get hurt... the mare, however, certainly deserves everything I can give her at this time. She is usually quite sweet, rather maternal, but this morning, I tried to gently "check" her for milk production and she turned with open, barred teeth towards me! I let her nose "run into" my fist and she backed off; then continued to act "offended and annoyed" for a bit, including one more attempt to bite me. Finally, she became sweet again and accepting of me rubbing her neck and shoulders. Training all of these ex-PMU mares will prove to be very interesting and complicated, no doubt! Dr. O, As always, thanks so much for your information and, believe me, I am very fretful over this mare's (and her unborn foal's) situation right now. I agree that bone infections often require prolonged antibiotic therapy for "sterilization" and, fundamentally, this lesion and the decayed, broken tooth need surgical intervention. The mare's mandible continues to drain, but not very effectively based on the amount of soft tissue swelling and ? boney distortion that I can see... it STINKS (I assume it is the smell of necrotic bone) and she absolutely will NOT let me clean it more than very gently applying a gauze with some H2O2... clearly, not very effective. Today, she completed 8 days of antibiotic therapy; I plan to go through day 10 and then my local vet will be out that day to give immunizations, possibly debride the wound again following some sedation. She is grazing on whatever is green and growing at this point in time; all three of the my ex-PMU mares are still in "quarantine" and being held in an enclosure that is about 300 ft x 150 ft. The have unlimited timothy/orchard grass hay available and, in addition to grain, they are getting a really good looking alfalfa/orchard grass hay mix twice daily. So, is she getting enough folinic acid... probably not... I know that the equine surgeon felt strongly that we should wait until 60 - 90 days post foaling for the surgery, but frankly, I'm not sure the lesion will wait that long... I just think she's loosing more and more of her mandible each day. If we can just get through her foaling, hopefully in the next 4 weeks, then maybe we can consider surgery a bit sooner than the timeframe he suggested. Maybe I'm just an anxious horseowner! And finally, for everyone who's been following the thread, here come the xrays. Hopefully, they will have enough resolution for everyone to see the lesion and the radio-opaque dye which shows the communication between the lesion and the third premolar tooth. I'll keep everyone updated. Martha 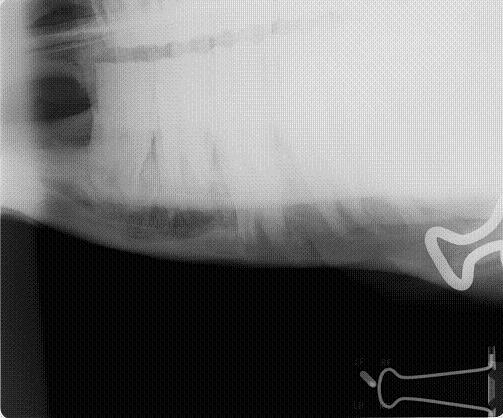 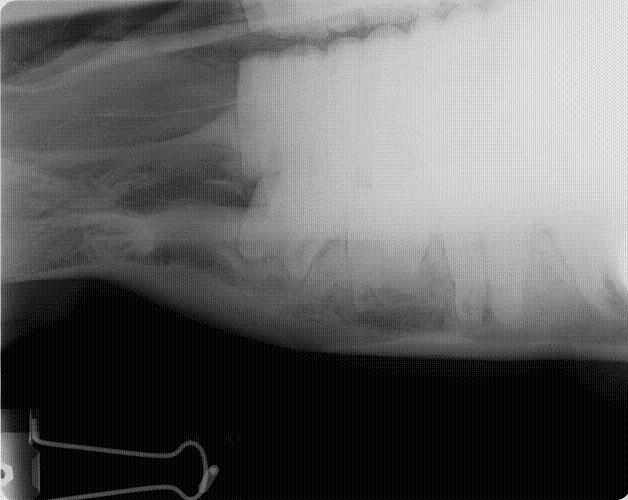 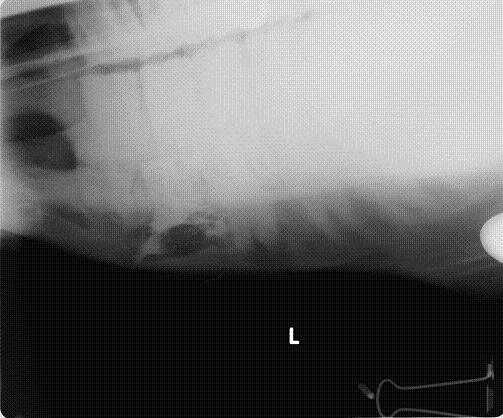 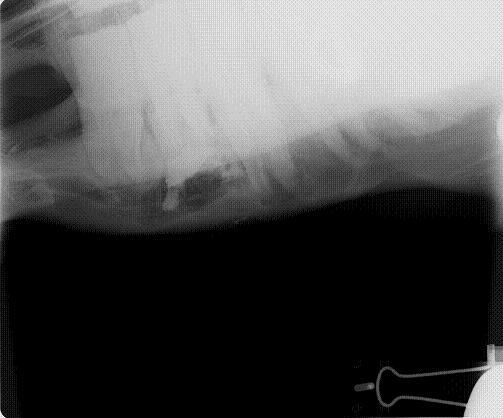
|
| Member: paul303 |
Posted on Monday, Apr 2, 2007 - 1:25 am: Boy, that is nasty. It almost looks like there is a possibility of involvement of the adjacent teeth. No wonder this mare is reluctant to have you work around her mouth. If the fistulas remain open and draining until she foals, she should be OK. Best of luck! |
| Member: zarr |
Posted on Monday, Apr 2, 2007 - 11:17 am: Martha that is just about where Goldie had her jaw broken and as I said TIME did heal. And isn't anxious horse owner our "middle names" ??!! You are doing such a wonderful thing can hardly wait for baby pics! Cindy |
| Moderator: DrO |
Posted on Tuesday, Apr 3, 2007 - 6:41 am: The odor Martha is probably the decaying food lodged in the fistula in combination with the mouth's anerobic bacteria. Though I don't often recommend this, I wonder if the horse would allow a hyDrOgen peroxide with betadine flush daily? If so see if your veterinarian would approve such a flush.DrO |
| Member: mitma |
Posted on Friday, Apr 6, 2007 - 11:44 pm: Hey Everyone,Sorry it's taken me so long to get back to you all... First, Dr. O, my mare (Mitzee) definitely does not allow much, if any, contact with the affected area. The first day that my local vet came out to see her, when he had to sedate her to adequately exam, then irrigate, the wound, he left me the betadine wash solution in hopes that I could do wound care each day, but, sadly, it has remained on the shelf. The most I can usually do is "dab" the wound with H2O2... Meanwhile, the final culture grew out Streptococcus equisimilis. We finished our 10 days of trimethoprin/sulfamethoxazole antibiotics and, interestingly, 48 hours later (last night), Mitzee had further developed a large, very angry looking "pustule". It was about the size of a ? lime and really quite elongated out from it's origin. Unfortunately, at the time, I didn't have my camera with me, but tonight I took the pictures that follow below (sorry for the obvious "grossness"). You can see that the area has spontaneously drained once again, but the surrounding soft tissue distortion and obvious lymph node enlargement is really remarkable to me. I just want her to foal SOON so she can have a general anesthetic for removal of the tooth remnant and the debridement of the mandible in a proper fashion! YIKES!!! Stay tuned! Martha     
|
| Member: mitma |
Posted on Thursday, May 17, 2007 - 1:25 am: Dear HA Friends,I just wanted to give everyone an update on my ex-PMU mare, Mitzee, who had the mandibular abscess we discussed several weeks ago. Well, Mitzee (a varnish roan appy bred to a very loud leopard stallion) foaled a healthy SOLID bay colt on 4/24/7 (I also had a thread about her ensuing labor and ongoing tachycardia issues). She fooled us regarding her labor, so we missed the delivery. My vet saw her and the new foal that morning that I discovered them and said everything looked O.K. We had talked previously regarding the fact that we wanted to schedule surgery as soon as possible (though the consulting equine surgeon had suggested we wait until the foal was 2 - 3 months of age), because this poor mare had continued to have significant swelling under her jaw which intermittently drained really disgusting material and reeked of decaying, necrotic, infected flesh. No doubt, though she continued to feed well, she probably was experiencing some discomfort. Anyway, my vet called the surgeon and we arranged to have her surgery yesterday! Everything went extremely well, though the procedure was more difficult and more time consuming than expected. The surgical team incised the soft tissue area (shown in previous posts), extensively debrided the affected area of the mandible, as well as the two communicating tracts leading to the abscessed tooth root; repulsed the broken, decayed tooth; then filled the tracts and the mandibular bony defect with antibiotic impregnated bone cement. I was able to be present during induction of general anesthesia (because I was holding/entertaining baby Rorie near his mama while she fell asleep) and from the perspective of a human anesthesiologist, I now have even more respect for everything our wonderful equine vets do for our precious horses. It was truly amazing to watch a 1000+ lb animal safely taken into the "reversible coma state" and then MOVED onto the operating room table. WHEW!!! The surgery took almost 4 hours but Mitzee recovered pretty fast; once upright again, she was intent on getting back to her foal (I found that during the four hours, my loving care of Rorie was inadequate to keep him "safely" calm enough while we waited, so he had to get a little sedation also... he was literally climbing the stall walls after about an hour into the ordeal!). I have attached pictures taken about 30 - 45 minutes after Mitzee returned to the stall with Rorie; when he saw her, he latched onto her teat and did not stop nursing for quite a while; it was really comical and endearing to watch. I brought them both home today and though Mitzee is still less interested in eating grain, she consumes hay voraciously. Mitzee's future may still be uncertain; I sincerely hope that ALL the infection has been eliminated, but I know how difficult this lesion was for the surgical team and only time will tell! She will return to the clinic for a followup visit in 1-2 months, especially for xrays to check the integrity of the mandible. I'll keep everyone posted. Thanks! Martha P.S., Dr. O... surprisingly Mitzee's heart rate was 40 this morning which was the lowest it's been since I've been checking it for the past 3 - 4 weeks. YEAH!!! My vet and I have discussed this issue several times and since this mare had always been afebrile, eating well, showing evidence of good perfusion, etc..., we continued to observe her... so it was bothersome, but a bit of a mystery. Now, I can't help but think that part of the elevation was due to pain???   
|
| Member: canter |
Posted on Thursday, May 17, 2007 - 7:59 am: Hi Martha,Thanks for sharing the good news on a successful outcome. Poor Mitzee has really been through a tough time - I'm so glad she found a loving home to take such good care of her. Will continue to keep fingers crossed that there are no more issues with her jaw and that the healing goes well. |
| Member: dres |
Posted on Thursday, May 17, 2007 - 9:43 am: Martha this mare is so lucky to have found you .. The colt already shows a app characteristic of the 'human' eye, sclera.. I bet with time you will see some appy roaning and other characteristics showing / molting / striped hoofs.. He will bloom...Keep us posted on the mare and him... On the first day God created horses, on the second day he painted them with spots.. |
| Member: terrilyn |
Posted on Thursday, May 17, 2007 - 9:55 am: Congratulations Martha...what good news! Look forward to seeing you soon!Terri |
| Member: hwood |
Posted on Thursday, May 17, 2007 - 9:59 am: Amazing account, Martha. Will you be taking her temp every day before the next check-up with the vet? I would worry that it was too long a period to wait to see if all the infection was cleaned out, but I expect she's on some pretty powerful anti-biotics, too, eh?Glad these two found a home with you. You certainly have your hands full!! |
| Member: paul303 |
Posted on Friday, May 18, 2007 - 12:19 am: Thanks so much for the update! It would seem that Mitzee has been fighting this infection for a LONG time - on top of carrying a foal. That's a pretty tough mare you've got there. In general, the mouth usually exhibits some pretty amazing healing powers. I'd agree with Holly to watch carefully for any signs of infection, but I really don't think I'd be all that surprised if Mitzee sails right through. |
| Member: mitma |
Posted on Friday, May 18, 2007 - 12:27 am: Thanks for everyones' heartfelt support... I will definitely keep everyone updated as things progress with this mare.BTW, Holly, I do NOT plan to take her temperature everyday, because this mare has a mind of her own and her back end is still a danger zone as far as I'm concerned! What I do with her each day depends on the amount (if any!) of help I have trying to care for her. For example, our equine surgeon suggested I change her dressing (the one you see in the previous pictures) every 1 - 2 days... you know, depending on how things are going. Since I just brought her home yesterday, I had hoped to wait until tomorrow before tackling the dressing... not only does it involve removing the sticky elasticon bandage and replacing the sterile gauze 4 x 4s over the incision site, but it also involves removing/replacing a betadine soaked gauze strip that has been "packed" into the soft tissue defect overlying where the anitbiotic impregnated bone cement was applied to the mandibular defect created from the abscess. Now, since this mare doesn't tolerate being in a stall for extended periods of time, she and baby Rorie live in our riding ring (kinda like a partially dry lot) which is rather large and has an attached run in shed. Last night, we got quite a bit of rain in central Virginia, so I knew I would probably have to deal with her dressing today, as she undoubtedly stood out in the rain most of the night and a wet dressing might encourage more bacterial contamination. Now, I had an experienced horse person with me today, but it was still an ordeal to remove the elasticon and gauze 4 x 4s. This process took almost an hour and involved a little bit of rearing and running us into the walls of the large stall where we were performing this task. Once the dressing was off, I decided that there was just NO WAY I would try to further remove the betadine soaked gauze strip. We managed to finally get sterile gauze pads back on the incision area and wrap her head with more elasticon. Whew! After that, I caved in and called my regular vet who, now, is coming out in the morning and will probably sedate her so we can do more effective dressing changes and wound care. I also hope that we can figure out a reasonable plan to get her through the next few weeks while she heals. I certainly don't think he should or will come out every other day to do the dressing changes for me, though that would be very nice!!! Also, though Mitzee is eating her hay quite well (and I do have some lovely, nutricious alfalfa), she really doesn't show much interest in her grain, so I need to figure out a mash that she might eat, if for nothing more than I would like to continue giving her Bute for a few days... Despite my hands being quite full, this is also a wonderful experience that is teaching me an incredible amount of valuable information (which, no doubt, I will use on the next pregnant, ex-PMU mare I adopt!)... Martha |
| Moderator: DrO |
Posted on Friday, May 18, 2007 - 6:15 am: In general Martha head wounds, and wounds of the mandible heal better than other places on the horses body. I think it is because of the rich blood supply. This is combination with the extensive debriding and removal of the focus of infection suggest to me a very good prognosis. Thanks for the update.DrO |
| Member: mrose |
Posted on Sunday, May 20, 2007 - 6:00 pm: Martha, a wonderful job done by you and her vets! The foal looks great; and look healthy as can be. He's a big guy, too! How tall is his mom?I'm betting on healing with no problems. 
|
| Member: mitma |
Posted on Saturday, May 26, 2007 - 8:48 pm: Greetings HA friends,Just thought I would let everyone know that Mitzee has had a bit of a set back. As you know from my previous posts, postop wound care and dressing changes have been a challenge. My incredibly wonderful local equine vet has been coming out to help, each time Mitzee was sedated and things really go much better that way. Well, initially he came out last Friday (8 days ago), which was POD # 3 for Mitzee. Two days after that Mitzee completely dislodged her gauze dressing, which I then kind of "patched" and at that time, I noticed a fair amount of serosanguinous drainage on her external stocking dressing which we had fashioned for her to wear like a fly mask, in order to help keep the gauze in place with less elasticon. I thought "oh well, I'll just watch this". Two days after that, my local vet is out and everything gets redressed/rebandaged nicely and at that time, the most superficial soft tissue defect looks O.K., with some obvious granulation tissue present... Well, later that evening Mitzee, again, completely dislodged her dressing which I "patched" again! She is really a "Houdini" and has taken to rubbing on anything, including baby Rorie!!! Innocently, I thought she might be rubbing alot, because healing wounds are often very itchy! Now comes the nightmare... I was out of town on Thursday, so when I got out to see her Friday afternoon (and my vet was meeting me out there), I couldn't believe it... she had a HUGE area of swelling visible under her external stocking (clearly, she again rubbed out the gauze from my patch job) similar to what her mandible looked like well before her surgery. The most impressive thing was when I got within about 15 feet of her, the ODOR hit me!!! At that moment it occurred to me that we probably didn't get all of the infected bone debrided during surgery. When my local vet arrived he was just amazed and while he clean and irrigated the area, I called the equine clinic where she had surgery. Earlier in the week, I had talked to our surgeon and I knew he would be out of town for the holiday weekend, but the on call vet said to bring her up and that's what we did last night. Currently, all the sutures and staples have been removed and the new abscess has been irrigated several times (with sedation). She was started on PO metronidazole (Flagyl) and she's on higher doses of Bute to help with all the inflammation present. This morning after she was sedated it became apparent that this new abscess area does communicate with her oral cavity, apparently through a ?separate defect in her mandible. In this setting, I'm so worried that given the initial size of her mandibular lytic lesion, she's at risk for a pathologic fracture, but she is eating pretty well, both grain and hay, so I guess her jaw is working. What an absolute nightmare, but I am committed to seeing this through... our surgeon will return next Tuesday, so I bet we'll be back in operating room for more surgery pretty soon. I'll let you guys know how everything goes. Martha P.S., I thought about taking some pictures, but didn't get around to it with everything going on, but this was even more gross than before! |
| Member: mrose |
Posted on Sunday, May 27, 2007 - 1:10 am: Oh, wow Martha! I'll be anxious to hear what the surgeon has to say. Maybe he can deal with this without more surgery. Let's hope so. Good luck, and kudoos to you for sticking with this mare. |
| Member: paardex |
Posted on Sunday, May 27, 2007 - 6:43 am: I am so sorry ,sometimes you really do not get lucky do you?I'll keep my fingers crossed for you and Mitzee. Jos |
| Member: frances |
Posted on Sunday, May 27, 2007 - 7:22 am: Oh no, just when things were looking so good. What a shame. Very best of luck. |
| Moderator: DrO |
Posted on Sunday, May 27, 2007 - 8:59 am: Hello Martha,I know such back steps are discouraging but in problems of this nature they are common and even expected and the trick is to deal with them one at a time. I would say one of the keys to avoiding such problems is finding some dependable way to keep the wounds clean enough to not smell. Has no one yet approved the use of a antiseptic/peroxide mixture to clean out the wounds contaminated by the oral cavity? Do they believe it will interfere with bone healing DrO |
| Member: zarr |
Posted on Sunday, May 27, 2007 - 11:50 am: Martha sad to hear of the set back it does seem for every 1 forward 2 slip back but your determination and Mitzees will I hope it changes direction and healing begins soon. I told you about the morgan mare I worked with and it was up and down but in the end she was alright. Mitzee is receiving MUCH better care than Goldie every did ! Cindy |
| Member: mitma |
Posted on Sunday, May 27, 2007 - 10:57 pm: Thanks everyone for all the well wishes...And Dr. O, I know that these events can be pretty common... I think I was just taken back as to the incredible change that had occurred from Wednesday to Friday with regard to the size of the "new abscess" and the odor emitted, plus I was really tired, so my frustration was showing. For now, the on call equine intern (who seems very competent and skilled), plus the internal medicine equine vet have been managing Mitzee as an inpatient; she's definitely getting daily, if not twice daily wound care, as well as the meds I previously mentioned. I don't know for sure, but I think they're irrigating the wound with a dilute betadine solution, but perhaps it's something else. I know that at the time of her initial surgery, the surgeon felt that "sealing" off the oral cavity with the use of the antibiotic impregnated bone cement was a priority. My local vet, as well as the two at the equine clinic that I just mentioned, do think that this new abscess represents a "left-over" area possibly missed during the surgery, rather than a new postop infection. The surgeon will return this Tuesday, so I'll have an update then. I will say that just two days now of intensive wound care have improved the look of the wound tremendously and Mitzee is eating well and, otherwise, looks O.K. Thanks again! Martha |
| Member: paul303 |
Posted on Sunday, May 27, 2007 - 11:10 pm: There is a product ( perscription ) called Peridex. It is a chlorhexidine rinse. |
| Member: mitma |
Posted on Thursday, May 31, 2007 - 2:36 am: The plot thickens, or should I say, worsens???Mitzee had some additional xrays yesterday (sorry, I don't have them yet, nor have I actually seen them) and it appears that the adjacent tooth (I assume the lower 4th premolar) does show signs of tooth root infection. Now, doesn't a "bad tooth" need to be removed??? Clearly, the infection has extended through the mandible to the underside of her jaw area as that's where it's draining... At this point in time, the surgeon seems to want to treat somewhat conservatively, i.e., non-surgically. One of the possibilities suggested was hyperbaric oxygen therapy. So, I did some research and it appears that there are two chambers near Virginia, one at the UT Knoxville and one, someplace in Maryland though I haven't been able to determine if it's an academic center or a private clinic. (Did you know that there is a Veterinary Hyperbaric Medicine Society??? Also, I found another interesting website, www.equinehyperbarics.com...) Now, I think that evidence-based medicine is pretty important and I did a search on pubmed.org using the terms "hyperbaric oxygen therapy" and "horses/equines/veterinary medicine" and NOTHING relavent showed up... can it be that this modality has actually not been studied in horses??? Dr. O, I would really appreciate your thoughts here... It seems to me that the options are as follows: 1-More Surgery (oral extraction vs. repulsion of the affected tooth vs. periapical curretage without extraction??); 2-Medical therapy with ?antibiotics, ?anti-inflamatories, aggressive wound care, etc...; 3-Add Hyperbaric Oxygen therapy to either option 1 or 2, or 4-Do Nothing. Thanks for any thoughts! Martha |
| Moderator: DrO |
Posted on Thursday, May 31, 2007 - 5:50 am: I presume from the history the rationale for the hyperbaric oxygen is the presence of anaerobic infection. This is a legitimate use as these organisms do not do well in a oxygen rich environment.However to maximize the effect of such treatment I would first make sure any infected tissue is aggressively debrided to remove dead/infected tissues and reassess the daily treatment plan including the antibiotics used. If your current veterinarian seems reluctant to aggressively remove infected tissue, there may be a reason you don't state but if it does not make sense to you consider a referral. Following such work, hyperbaric oxygen could be considered. DrO |
| Member: canter |
Posted on Thursday, May 31, 2007 - 8:04 am: DrO, As I read through Martha's case, a thought occurs to me but I have no idea if this has any sort of application in horses: my dog was a year old when diagnosed with cancer of the jaw. It was so aggressive that we had no choice but to have a part of her right lower jaw removed. We were fortunate to live near Tufts at the time. Thirteen years later, my dog is old and slowing down but thrived all these years without 1/4 of her jaw.Going back to Mitzee, while I realize that Martha's mare likely doesn't have cancer, "just" this very nasty infection, if the vet can't get a handle on it, is a partial mandablectomy (I'm sure I hashed up that spelling) an option for Martha before further damage is done? Obviously the anatomy of horses and dogs is quite a bit different and the risks of putting a horse out for surgery are great, but I was just wondering about this as an option for Martha's mare. |
| Member: mrose |
Posted on Thursday, May 31, 2007 - 11:53 am: Martha, with people when an decayed tooth isn't treated, The decay will eat down into the root canal and abcess, and then will eat into the jaw bone. Also, if the tooth isn't removed it will affect the tooth next to the decayed or infected side of the tooth and spread. Once into the jaw, if not stopped, it can eventually eat away much of the jaw as well. The infection will also often enter into the blood stream and cause a systemic infection. Usually, with people the infection itself will respond to penicillin; but at the same time the patient is put on penicillin, the affected teeth must be removed. Normally the pain is so great that people see their dentist before the infection spreads very far into the jaw bone. However, I did see one case where the jaw was severly affected, and the patient had to go into surgery and have about an half inch of jaw bone drilled out and filled with bone cement. Just going by my experience with humans, it sounds like this might be what your mare needs. Infection of the bone is very difficult to controll without removal of the decayed bone.As to the hyperbaric chamber treatments, they could be benificial, imo, even if the bacteria isn't anaerobic because it will increase the oxygen to the red cells and promote healing. However, imo it should be used in conjunction with oral surgery, unless there is some reason not to do the surgery that isn't mentioned above. Libby, my mare that had the severed tendon then got a severe infection that involved her sesamoid bones as well as tissue did not respond to antibiotics, even though she was on strong doses given IV. She had 4 hyperbaric treatments and imo and that of her vets, that is what saved her life. However, she also did have to have surgery first to removed infected bone. After her second hyperbaric treatment there was a marked difference. I think the website of the clinic she went to has info on the hyperbaric treatments at www.alamopintado.com Good luck with this mare; she's lucky to have you! If this were my mare, I'd try and find an equine oral surgeon, if there is such a thing, or |
| Member: paul303 |
Posted on Thursday, May 31, 2007 - 9:58 pm: Yeah, Martha, an infected root does need to be removed. I posted before ( right after you posted the x-rays ), that it looked like the adjacent teeth were involved. The most basic thing to be done is to remove the source of the infection. Any time the fistula stops draining, the whole area ( tooth and jaw ) will be too painful to use, and an active infection always leaves you open to septicemia or cellulitis. The hyperbaric treatment is interesting, but let's face it: that tooth is not essential for life. In the last two x-rays you posted, it looks like the infection involves 4 teeth and possibly a fifth. An infected tooth ( nerve ) doesen't get better, so unless there are equine oral surgeons that do root canals and apicoectomies ( removal of the root tips ), removal of all the affected teeth seems the most reasonable treatment. |
| Member: mitma |
Posted on Saturday, Jun 2, 2007 - 10:11 am: Hey Everybody,Sorry it's taken so long to respond, but I'm being held hostage at work this week. Let me just say that most of what I know about human medicine and the pathogenesis of an abscess argues to remove the infected tooth, as well as extensively debride the affected mandible and affected soft tissues. However, I have had long conversations with my equine surgeon (and he seems to be a reasonable, logical practitioner who is a board certified, ACVS surgeon, previously practicing in an academic center) as well as my own ambulatory vet; the surgeon has spoken with his partners, including one who has a practice focus on equine dentistry, and the bottom line is that he wants to wait a minimum of 30 days before attempting further surgery. His rationale is that the the first surgery was extremely difficult, there has been insufficient time for adequate healing of tissues, and further debridement of the mandible and/or tooth removal vs. periapical curretage vs. some kind of endodontic procedure (root canals, etc...) at this point in time would put Mitzee's mandible at risk for an iatrogenic fracture and may not even accomplish the desired resolution of the abscess. He believes that systemic antibiotics and good wound care will allow for adequate healing from the previous surgery and also keep the current 4th premolar tooth root infection from progressing and possibly, may partially/completely treat it... I am willing to see how things go for a few days, even maybe a week, but in order to pursue this conservative course of therapy, I will need to see objective evidence of improvement. In the absence of that, i.e., if further or worsening purulent drainage and/or edema formation continues from/at this soft tissue tract under her mandible, then I will probably pursue other opinions. And, that brings me to my project this weekend... am researching the existence of equine oral surgeons; so far, I have found lots of equine dentists and equine vets who specialize in dentistry, but not an equine surgeon who specializes in the oral cavity. If anyone knows of one or an academic facility that has/is focusing on this area, let me know. Finally, we have done another contrast fistulogram, but because of my work schedule, I haven't spoken to the surgeon yet about the results; also, culture taken last week is probably back, but don't know those results yet. I'll keep everyone posted. Thanks alot! Martha |
| Member: paul303 |
Posted on Saturday, Jun 2, 2007 - 9:01 pm: I see the reasoning behind the treatment. Hopefully, the antibiotics will create some improvement in the situation. Much luck to you, Martha! If there should be anymore x-rays, do you think you could post them? |
| Member: mitma |
Posted on Sunday, Jun 24, 2007 - 3:39 pm: Greetings Everyone,I have finally received some of Mitzee's xrays, though it appears that I'm missing several... hmmm... Anyway, I thought I would give everyone an update. After two weeks of inpatient care (IV antibiotics, anti-inflamatory agents, a few different wound site I&Ds, several xrays and another fistulogram, etc...), she was discharged on 6/7/7. The final fistulogram showed NO evidence that the draining sinus tract communicated with the adjacent tooth root (4th premolar), but, rather, seemed to travel to the empty alveolar socket of her previous surgical site (the removed 3rd premolar). I had decided I did not want to attempt to manage her on my own, so I arranged to board her and Rorie at a facility owned by an equine vet, kind of like a lay up hospital situation... She's been getting daily assessment and care of her wound, the barn has a great fly control system and, so far, she usually goes out at night and stays in during the hot day. Plus, when she and Rorie are out, they're with other mare/foal pairs and that's a nice bonus for Rorie. Mitzee's eating well, her weight is good, and her activity is normal. And, though tissue healing is occurring, significant swelling of her left submandibular area persists and there are two remaining tracts that drain purulent material, though it is less than previously observed. I have decided to see how things go for awhile and "embrace" this conservative approach... clearly, the surgeon was not interested in pursuing more surgery at the time of her discharge, though when I corresponded with him recently (and showed the same pictures I am posting below) he suggested we get a CT scan. Of course, a CT scan appears to require general anesthesia and I would have to take her to a larger referral, probably academic, center. Based on where I am in VA, the closest facilities are NC State in Raleigh, NC, Marion duPont Scott in Leesburg, VA, or VA Tech in Blacksburg, VA... I do still worry that there's something "left behind" in the wound, perhaps a necrotic bone fragment???, that is continuing to feed this low level infection... At this point in time, she is almost 6 weeks postop from her initial surgery to remove premolar #3... Rorie was 8 weeks old last Tuesday... What does everyone think???? Thanks! Martha    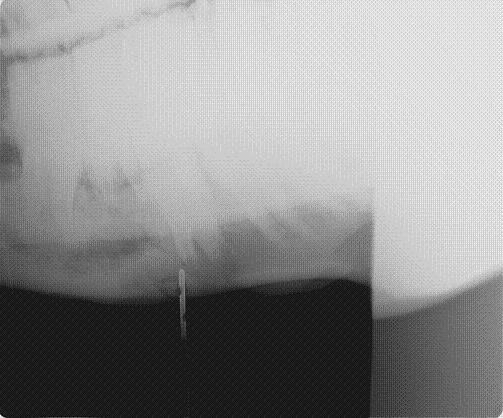
|
| Member: mitma |
Posted on Sunday, Jun 24, 2007 - 3:49 pm: Oops... forgot to show this picture of Mitzee and Rorie visiting with a nice (but dominant) warm-blood filly the same age as Rorie... At least Rorie is being submissive with her, because he chews constantly on Mitzee, mounts her, and, in general, is a menace! She very patiently ignores everything, so when I work with him, I have to spend alot of time reminding him that I'm the boss!
|
| Member: zarr |
Posted on Sunday, Jun 24, 2007 - 5:29 pm: Martha, think I see more Dennis the Menace than submissive in those ears & eyes! I would worry with that swelling also but if there is not much heat ?? Goldie's took a lot of time. She looks SO GOOD! Cindy |
| Member: mrose |
Posted on Sunday, Jun 24, 2007 - 6:44 pm: I'm so glad things are looking up for this mare! She's got a real cutie of a foal; and I agree with Cindy on his look! |
| Moderator: DrO |
Posted on Sunday, Jun 24, 2007 - 7:09 pm: I presume the folks who look at the original and complete set of radiographs, see no dead bone? Martha, considering everything, the swelling itself is not a bad sign and may take time to resolve. The radiograph is difficult to evaluate as it seems to lack much detail, possibly a problem with the generalized swelling. The parts we can make out look ok. Most important their is still purulent drainage, indicating the bodies attempt to rid itself of infection and/or necrotic material. As long as it is improving the conservative approach may work.DrO |
| Member: mitma |
Posted on Sunday, Jun 24, 2007 - 8:57 pm: Thanks Dr. O and Everyone,Sorry, I know the film is somewhat poor... the surgeon's office girl sent me several films via an email attachment, so I wonder if when I downloaded them and reduced their sizes maybe I lost some resolution??? Hopefully, I will get a CD of all these films and can post better copies for your review... The surgeon reviewed all the films with me on the day of Mitzee's discharge and he felt pretty comfortable with everything being O.K. at that time, but, recently, when he saw the pictures I posted above, he suggested we get a CT scan... Dr. O, what's your take on that???... and, BTW, since you're in NC have you had "experiences" with NC State's vet school??? They're only down I-95/I-85 about 120 miles or so from Richmond and it would be a manageable trip to make, if needed... Regarding the issue I raised previously about hyperbaric oxygen therapy, I did talk to UT Knoxville and found out that their old chamber (a portable one) is not operational now in order to be replaced with an upgraded chamber (one that is permanently in place), hopefully sometime by the end of July... So, if there's ongoing evidence of infection, I still want to keep HBOT in mind... Thanks! Martha |
| Member: paul303 |
Posted on Monday, Jun 25, 2007 - 1:39 am: The picture quality IS poor, but it almost looks like there is some healing going on. |
| Member: mitma |
Posted on Thursday, Dec 27, 2007 - 10:48 pm: Hey HA friends,Just wanted to say that Mitzee and I have arrived in the Tarheel state tonight! In a nutshell, for the past several months, Mitzee has continued to have intermittent serosanguinous vs. scant purulent drainage from her submandibular area and a significant ?fibrosed deformity of her jaw, though really no other indications of clinical problems... she's chewing well, weight is good, afebrile, etc... Sometime back in the summer, our equine surgeon had suggested that we undergo a CT scan (you guys may remember that even though Mitzee had significant purulence and edema following her initial surgery in May, the surgeon was very reluctant to "re-explore" the area due to the difficulty of that first surgery and the lack of evidence from her contrast fistulograms that the adjacent tooth root was involved in any infection)... So, though I had hoped to have her undergo this in the summer, NC State's Vet School was awaiting a "functional" table to use for equines in the scanner; and, though I was considering going to VA Tech instead, I had that little foot fracture in July which pretty much impaired my equine activities for several months. Given that she looked so good clinically, I decided to wait for NC State's table to be operational, but also given the continued appearance of the submandibular drainage, I still wanted to rule out any retained ?necrotic bone fragment or area of osteomyelitis in her mandible. So, tomorrow is the big day for the CT scan. The CT scan findings will direct any subsequent care, more surgery vs. medical therapy vs. nothing needed... I hope to get the CT films and post those sometime this weekend... wish us luck! Martha P.S. And, BTW, the other really wonderful thing is that I weaned baby Rory about a month ago (I changed the spelling of his name when I submitted his registration papers)... and in doing so, I moved Mitzee to another facility; well, I've spent alot of time with her over the past month and we have actually started to bond; she clearly has begun to trust humans and, in particular, me! Just the fact that I can groom her completely, touch every area of her face/head, even the submandibular area without too much protest, pick up her hooves (briefly) is all really wonderful! The new barn where I'm boarding her is a very busy hunter/jumper/eventing barn that gives a huge number of lessons, primarily to kids; Mitzee has really gotten desensitized to all the chaos that goes on and all the little girls at the barn just love her (she is the only Appaloosa there and her "rescue" history has made her interesting to everyone there)... I have really begun to marvel at the smarts this mare has and how willing she is to tolerate many different situations; I really believe that she will be under saddle in the next several months and that she will make a wonderful and safe mount! |
| Member: zarr |
Posted on Friday, Dec 28, 2007 - 1:09 am: Little girls are the best cure-all for troubled horses there is and the fact that she has seen you as someone she can trust is such good news. I don't care if its horse, dog ,cat or small bird who fell out of its nest when you realize that the gift of trust has been given it is the most wonderous feeling in the world! Best wishes on Mitzee's CT scan! Cindy |
| Member: canter |
Posted on Friday, Dec 28, 2007 - 8:37 am: Good luck on the CT scan, Martha. Hope all goes well and you find the answers to get this cleared up once and for all.And, Congratulations on making huge leaps and bounds on building trust with Mitzee. It's so gratifying to build that bond and you have a lot to be proud of. Hope your foot has healed well enough so that when Mitzee goes under saddle for the first time, it's your proud face we see a picture of from that saddle! |
| Moderator: DrO |
Posted on Saturday, Dec 29, 2007 - 9:43 am: Thanks for the update Martha and am surprised to hear you are having problems. The lack of problems on the last radiograph suggest this should have healed in most cases. There are two explanations:1) a foreign body, possibly a dead piece of bone 2) a resistant infection either bacterial or fungal Hopefully the CT scan will help better define the problem so it can be fixed but surgery with thorough debridement and good microbial work up are likely to be required whatever they find. Keep us appraised Martha. DrO |
| Member: mitma |
Posted on Saturday, Dec 29, 2007 - 8:14 pm: Well, thanks for everyone's comments!Here's the scoop... the CT clearly showed infectious "involvement" of the adjacent tooth (left lower 4th premolar), though fortunately, the root and the pulp appeared to still be healthy; also, an area of the mandible inferior to the previously removed tooth (left lower 3rd premolar) had a "sequestrum", sort of under the now empty alveolar socket, which is well healed. So, immediately following the CT, after the surgeon reviewed it with the radiologist, Mitzee got moved to the OR (still under general anesthesia) and debridement of the affected areas began. Once the surgeon performed an oral exam, he was also able to demonstrate an orocutaneous fistula, corresponding to the exact area on her lateral jaw where she has had continued intermittent drainage for the past several months. The surgery and anesthesia were uneventful and she looked great when I left her last night (I'm on call today at work)... I will probably be able to pick her up as early as tomorrow, but that will depend on how much sleep I get tonight. Hopefully, I will be able to post some pictures of her xrays and CT scan for everyone to see... NC State has this great program, called Amicus, that "converts" the two dimensional information from the CT scan into three dimensional, COLOR, pictures and WOW, what information they reveal... just remarkable (I doubt I will be able to post any of those pictures due to the licensing issues with the software company)... Also, the veterinarians and staff of NC State have been AWESOME... I'll try to post pictures tomorrow... Martha |
| Member: zarr |
Posted on Sunday, Dec 30, 2007 - 1:32 am: Such GooD news for both of you and yeah for the finding of the fistula they are often the underlying problem and not easily detected at least my own were not! Rapid healing to Mitzee and sleep to you! Cindy
|
| Moderator: DrO |
Posted on Sunday, Dec 30, 2007 - 8:25 am: That is most excellent Martha, I look forward to the images.DrO |
| Member: mitma |
Posted on Tuesday, Jan 1, 2008 - 11:08 pm: Hey Everyone,Sorry for the delay in posting the images... Mitzee was discharged on Sunday (POD 2) and I DrOve down to NC, picked her up, and travelled back to VA in the worst pouring down rain (not complaining, we still do have DrOught conditions a bit...) Anyway, I was on call the next day (New Years eve) and had a killer night, so I am still kinda brain dead today... I've managed to crash my laptop several times with the disc I was given at NC State... just wondering if it has anything to do with my new laptop OS, Vista, but now, finally, I've managed to load some of the study pictures onto my old laptop (hopefully the keyboard won't quit like it did this summer). The plain xray is not great... possibly me altering it in the download process??? Anyway, it is a lateral so you see both sides of the jaw and you have to focus on the near structures (the left side), not the far ones (the right side); basically, it shows distortion of the the left lower premolar #2, which has occurred following removal of #3 last May, and compensatory changes in the left upper arcade (see the big ramp/points above). The few CT views I've uploaded show extensive bony proliferation and periosteal reaction of the left hemimandible, an absent left lower 3rd premolar tooth, as well as some radioopaque densities below this area, presumed to be ?tooth fragments or cement debris following the previous surgery; there is one particular linear density located in the center of this area that was felt to represent a possible "sequestrum" and was removed... also, you can see a radiolucent tract that exits the lower portion of the left hemimandible below the empty alveolar area of the absent 3rd premolar. A lytic lesion is seen associated with the lateral aspect of left lower 4th premolar near the gingival margin and another draining tract travels between this front/rostral portion of the left lower 4th premolar tooth and the lateral aspect of the mandible; my discharge papers state that the CT findings "are consistent with peridontal abscessation and a draining tract", however the surgeon believes the root and pulp of the left lower 4th premolar tooth are still healthy, so we may have a ?50/50 chance of saving that tooth. I have also attached a few other pictures of Mitzee undergoing her CT scan under general anesthesia, her recovery from GA, and a view of the her face following the surgery where the diseased areas were debrided. Her discharge papers note the final diagnosis as "chronic osteomyelitis of the left mandible and peridontal disease adjacent to left mandibular premolar tooth #4". I'll keep everyone posted on her recovery. Thanks!!! Martha         
|
| Member: mitma |
Posted on Tuesday, Jan 1, 2008 - 11:15 pm: OK... despite my best efforts, only image 1 of 540 of the CT slices loaded, not 202, 205, and 215, like I selected... hmmm??? I really need to sleep now, so I'll work on reloading these images tomorrow... sorry!Martha |
| Member: juliem |
Posted on Tuesday, Jan 1, 2008 - 11:30 pm: Happy New Year Martha--what adventures you've had with this mare! You've been her savior for sure! Sleep well, Julie |
| Member: paul303 |
Posted on Wednesday, Jan 2, 2008 - 11:37 pm: Martha, you're incredible...thanks so much for taking the time. This entire process has been fascinating to watch. I must say that, despite all she's been through, your mare looks in great shape - an obvious testament to the excellent care you provide. |
| Member: mitma |
Posted on Monday, Jan 7, 2008 - 4:56 pm: O.K., I am going to try and load the CT images again... please refer to my descriptions of them above. Also, the surgeon from NC State called me today and reported the results of the cultures taken during surgery; Mitzee has grown two types of anaerobic, gram negative rod bacteria, a Prevotella "species" and Fusobacterium nucleatum. He said that he had not had a Prevotella isolated from equines in the past, but that the Fusobacterium is a common oral bacteria in a number of species.... Now, the plan had been for Mitzee to receive two weeks of postop antibiotics, trimethoprim/sulfamethoxazole (Bactrim DS) and when I brought her home on POD#2, I was able to give her the PM dose by syringing paste directly into her mouth (she did protest a little); for the next 24 hours, I was on call and during my absence the barn staff failed miserably in getting any drug into her! I certainly didn't want any of the barn staff to sustain injuries, nor did I want Mitzee to be hurt (apparently, she got into her rearing mode...), so I spoke with the surgeon then and he said I could forego her oral antibiotics (afterall, the surgical debridement was the "definitive" therapy!). Today, he mentioned that metronidazole (Flagyl) was the typical antibiotic for anaerobes, but that horses tolerate it even less than the Bactrim she had been on... so, since he felt good about the debridement, we are not treating her with antibiotics. The plan is to (as long as she looks good "clinically") take her back to Raleigh in about 4 weeks so he can examine her oropharynx and HOPEFULLY see that her orocutaneous fistula is HEALED and that the left lower premolar #4 is still O.K.!!! I'll keep everyone posted!Martha P.S. Keep in mind, when looking at the scans below, you are looking at a "cross-section" or axial image of the head, UPSIDE down... remember that she was laying on her backside to undergo the scan... also, the right side of the image is Mitzee's left side... notice the dramatic difference between the two sides, i.e., each hemimandible... 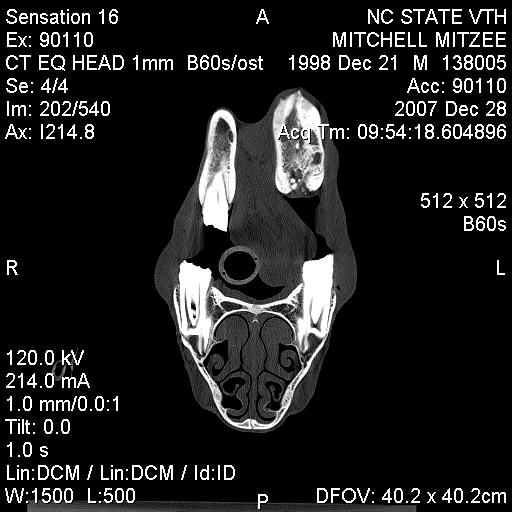 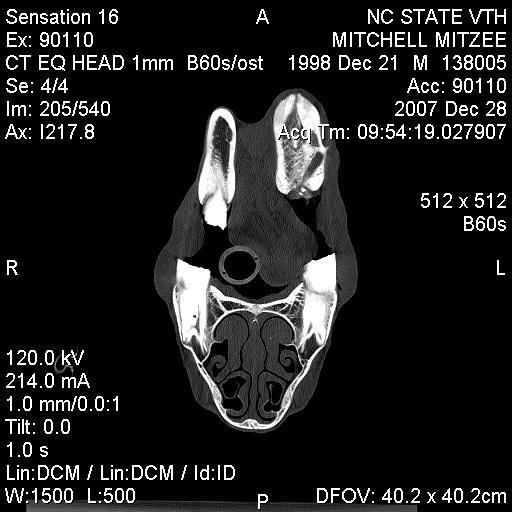 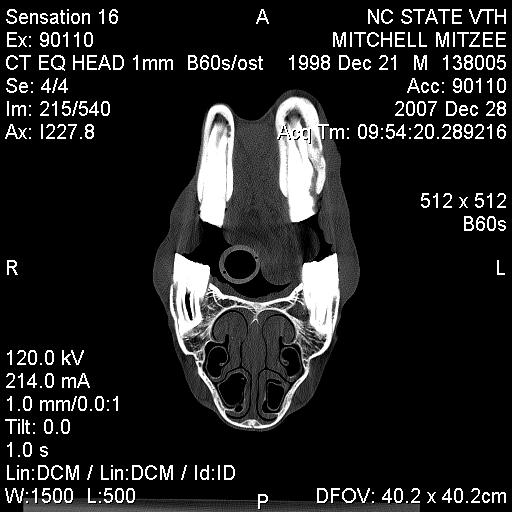
|
| Member: canter |
Posted on Tuesday, Jan 8, 2008 - 7:30 am: Martha, the pictures & images are remarkable. I know this has been a VERY long and difficult journey for you & Mitzee, but I really appreciate all the info you have posted.I'm keeping my fingers & toes crossed that Mitzee's latest treatment is the last one and she quickly makes a full recovery! |
| Moderator: DrO |
Posted on Tuesday, Jan 8, 2008 - 8:07 am: They really caught the fistula and infected mandible well. Good luck with the surgery outcome Martha.DrO |
| Member: paul303 |
Posted on Tuesday, Jan 8, 2008 - 10:01 pm: Wow! What incredible images. It's great of you to post this. Much appreciated. |
| Member: mrose |
Posted on Tuesday, Jan 8, 2008 - 11:00 pm: Wow, Martha! Great images. Really interesting. Thank you so much for posting these and for continuing to keep us updated. You've been through a learning journey for sure with this mare.I am certainly hoping that all is well with your mare and she has healed. You've been through enough with her! Please give us a report after your check up at NC. |
is The Horseman's Advisor
Helping Thousands of Equestrians, Farriers, and Veterinarians Every Day
All rights reserved, © 1997 -
