Site Menu:
| This is an archived Horseadvice.com Discussion. The parent article and menus are available on the navigation menu below: |
| HorseAdvice.com » Diseases of Horses » Skin Diseases, Wounds, and Swellings » Discussions on Skin Diseases not covered by above » |
| Discussion on Persistent Erythema Multiforme | |
| Author | Message |
| New Member: archemy |
Posted on Sunday, Apr 6, 2008 - 11:16 pm: I have an 8 year old Arabian gelding Rolin ((show horse )) who has had persistent Erythema Multiforme since early Feb (2 months now). Any ideas you may have would be GREATLY appreciated! )) who has had persistent Erythema Multiforme since early Feb (2 months now). Any ideas you may have would be GREATLY appreciated! I had had him for 10 mos when this began; he came to Colorado from Wisconsin. Prior owner/breeder had never seen this in him before. Initially we thought it was hives on his neck and flanks. Currently in a run with shed, blanketed, neighboring horses on each side. Wormed regularly every 2 months, up to date on vaccinations (last vaccines 9/07) History: 2/06/08 “Hives” noted on neck, flanks; saddle area spared. Dexamethasone 20mg/d begun. Treated for 3 days with complete remission of lesions. Previous weekly use of Shapley’s “MTG” to shoulders, hips, mane and tail halted. 2/11/08 Return of lesions covering entire body. Dexamethasone 20mg 3 days, 10mg for 3 days. Complete remission of symptoms again upon initiation of meds. Changed grass hay, stopped alfalfa, held monthly Adequan. Weight by tape 930 lbs. 2/22/08 Lesions returned more intensely, covering entire body. Several had begun to ooze. Seen by Lee Mueller, DVM. Exam WNL. Temp 99. Dexamethasone 20mg 4 days, 10 mg 4 days, then 10 mg qod with TriHist Bid. Again, Lesions abated within 24 hrs of 20 mg Dexamethasone. Training halted. (photos of horse with lesions and histology available) 3/2/08 Lesions returned on the first day off 10mg in the qod treatment. 3/3/08 Due to get 10 mg Dexamethasone after 1 day off; lesions back. Held Dexam. due to plan to take Rolin to Littleton Equine Hospital. 3/5/08 Seen by Dr. Bain at LEH. Extensive spread of lesions; oozing. Area on neck shaved, biopsied. Dx’d as Erythema multiforme. Erythematous collarettes with histology showing epidermal necrosis and large amounts of eosinophils. CBC and Chemistry normal. Started on Dexamethasone 20mg x 7 days, 10 mg x7days, then 7 days 10 mg qod. D/C Trihist. HyDrOxyzine 500mg tid for 3 days, then bid. Non-necrotic lesions resolved quickly. Crusted lesions cleaned with Benzoyl peroxide for 2 days. Continues on straight grass hay, stopped Strategy. Weight by tape 903 lbs. 3/16/08 Wormed with Anthecide. 3/25/08 Lesions return after 3rd off day; a few lesions were visible the previous day. Given dose of 10 mg as originally scheduled; added a second 10 mg. Lesions still palpable and visible at 5pm, gone by 7pm. Weight by tape 888 lbs. Discussed with Dr. Bain; consider allergy testing at CSU. 3/26/08 – 3/30/08 Lesion free while on Dexamethasone 10 mg and HyDrOxyzine 500 bid. Made appointment at CSU for skin testing; they only test for environmental allergens and require horse to be off of steroids for 4-6 weeks and antihistamines for 2 weeks. 4/1/08 Lesion free; reduced hyDrOxyzine to 500 mg q am. Healed ok from biopsy and normal horse scrapes. 4/2/08 Lesion free; reduced Dexamethasone to 8 mg qd. Started Milk Thistle detox supplement. 4/4/08 Small amount of nasal discharge. Hair is growing back on blanket rub spots and shaved biopsy area. 4/6/08 lesions returned moderately on neck. Given 20 mg Dexamethasone and HyDrOxyzine 500 mg. Nasal discharge gone. Vaccinations will be withheld. 4/7/08 Will go to Dexamethasone 10 mg and HyDrOxyzine 500mg qam with Milk Thistle. Post to Dr. Oglesby...Help!! Thanks, Arlyn}} |
| Moderator: DrO |
Posted on Monday, Apr 7, 2008 - 11:25 am: Welcome Arlyn,I do have a problem with the diagnosis of erythema multiforme because of the history and histology you provide. Though I have not seen a case of EM the literature states that the main cellular infiltrate should be lymphocytes and not eosinophils and the skin lesions not so rapidly responsive to treatment, usually days to weeks instead of hours. Your case reads more like a type 1 hypersensitivity. This results in urticaria (hives) and there are exudative and circular forms. However either diagnosis does not give you a actual cause, they are basically descriptions of the disease and in either case often an allergic response to some allergen is the reason. For initial therapy I would look to a combination of hyDrOxyzine and corticosteroid that aims at finding the lowest maintenance dose. This procedure is explained in Diseases of Horses » Skin Diseases, Wounds, and Swellings » Bumps / Nodules / Warts / Tumors » Hives, Wheals, and Urticaria in Horses. For long term control I would consider the procedure for identifying the cause in that article. You can shoot for intradermal testing but I have yet to see much information to recommend it as both false positives and false negatives are common. DrO |
| New Member: archemy |
Posted on Monday, Apr 7, 2008 - 3:06 pm: Thanks! I share your uncertainty with the diagnosis of Erythema Multiforme; I was unaware that hives could be circular.Attached are photos of skin lesions and histology. I have done as you suggested; we have a lowest maintenance dose of steroid and antihistamine. I will re-review your info on how to identify the cause. Thanks again! Arlyn  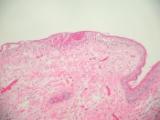 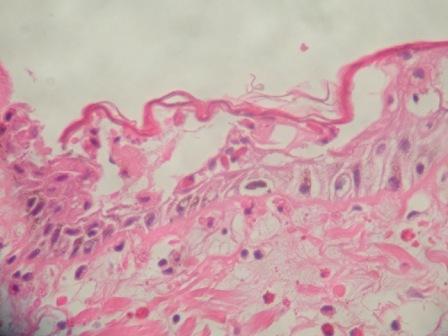
|
| Moderator: DrO |
Posted on Monday, Apr 7, 2008 - 10:34 pm: Remember the highest antihistamine dose should be used that does not cause sedation to try to get the lowest steroid dose. You should also note that it is not so much the amount of steroid as it is the frequency. Best practices are noted in the article referenced above. Every other day with Dex is probably not going to give the adrenal glands the stimulus needed to avoid adrenal suppression.DrO |
Horseadvice.com
is The Horseman's Advisor
Helping Thousands of Equestrians, Farriers, and Veterinarians Every Day
All rights reserved, © 1997 -
is The Horseman's Advisor
Helping Thousands of Equestrians, Farriers, and Veterinarians Every Day
All rights reserved, © 1997 -
