Site Menu:
| This is an archived Horseadvice.com Discussion. The parent article and menus are available on the navigation menu below: |
| HorseAdvice.com » Diseases of Horses » Eye Diseases » Anterior Uveitis, Recurrent Uveitis, Periodic Opthalmia, and Moonblindness » |
| Discussion on Treatment for frequent Uveitis - both eyes | |
| Author | Message |
| New Member: aanne |
Posted on Tuesday, Aug 31, 2010 - 7:22 pm: Hi Dr. O,My 4yr old horse was diagnosed with ERU (specifically anterior uveitis) a few months back. His history and now current attacks seem to verify this diagnosis. He unfortunately has this condition in both eyes. His first diagnosed bout received treatment for a month with atropine and topical maxitrol (dexamethasone/antibiotic). The dosage of the maxitrol went from a frequent 4 times a day application to twice a day, to once a day, then a complete stop after a month. He flared up in that same eye almost exactly one month later. I am concerned that perhaps he needed to be tapered off the drug..could that be a possibility for his relapse? If he does continue to get such recurrent bouts would you suggest keeping him on a once a week dosage of topical Corticosteroid? I should note that he is very responsive to steroid treatment. Would it be advisable to use the lowest concentration such as HyDrOcortisone once all inflammation has subsided? I’m worried about potential cataracts and glaucoma with long term use of a topical steroid, is this risk still associated with oral Prednisolone? Have you heard of any horses managed on the Alternate Day Therapy for uveitis? I prefer not to use bute since it masks lameness, but I am open to asprin – what is your current opinion of this treatment (I only see posts from 2004 on this topic)? What would be the suggested effective dosage for this type of therapy without the risk of stomach ulcers? Have you received anymore current information about the effectiveness on cyclosporin ointment? Additionally, his other eye flared up after he received a rabies shot. His other eye was already being treated at the time. Has there been any evidence that annual shots can cause flare-ups? Above all I’m looking for some way to keep away the uveitis since his outbreaks are so frequent. Please note that I'm not looking into surgical implants or any of those options - I've researched these and decided against them. Any information would be greatly appreciated! |
| New Member: aanne |
Posted on Wednesday, Sep 1, 2010 - 8:18 am: I have just had read on a different post where you had commented: Though most allergic disorders will respond to alternate day treatment autoimmune disorders have a reputation of worsening over time requiring larger and larger doses of medication.I assume then that prednisolone is not advisable? Additionally Benfotiamine has been big news in human uveitis treatment. Have you heard of this being used for equine treatment? |
| Member: andym |
Posted on Wednesday, Sep 1, 2010 - 11:12 am: A.AnneSorry to hear of your horse's uveitis. My TB mare has had uveitis in her right eye for about two years. A year and a half ago, I had a cyclosporine implant done at Ohio State U. Except for a month of healing, she has been without medications and without flareups since. My vet doesn't have the instruments to read the eye pressure which is a positive test for glaucoma. I found an equine opthamologist about four months after the onset. She found glaucoma had set in. She prescribed medications and advised me of the implant. I wish now I had found her sooner. It is my understanding that cyclosporine ointment cannot penetrate the eye so is not effective. I also found cosopt DrOps effective in reducing the eye pressure. Its prescription and used regularly by people with glaucoma. ERU can't be cured but can be medicated. |
| Moderator: DrO |
Posted on Wednesday, Sep 1, 2010 - 3:04 pm: Welcome A.Anne,I would recommend you try and find the minimum amount of topical dex treatment would be to prevent recurrence but cannot begin to guess what that would be. It seems unlikely that systemic steroid therapy is likely to reduce complications of steroid use. Individual cases are very different. There is no level of bute that is guaranteed to prevent stomach ulcers but the doses given in the article have been used without problems. I also give my opinion of NSAIDs in the article. As newer information becomes available we update the articles. As benfotiamine works by preventing glycation of tissues, and since this is not a known process involved with ERU, it seems unlikely to be of any use and I know of no work in the horse with it (see below for more). DrO The multifaceted therapeutic potential of benfotiamine. Balakumar P, Rohilla A, Krishna P, Solairaj P, Thanga Thirupathi A. Department of Pharmacology, SB College of Pharmacy, Sivakasi 626130, India. Abstract Thiamine, known as vitamin B(1), plays an essential role in energy metabolism. Benfotiamine (S-benzoylthiamine O-monophosphate) is a synthetic S-acyl derivative of thiamine. Once absorbed, benfotiamine is phosphorylated by ecto-alkaline phosphatase to lipid-soluble S-benzoylthiamine. Transketolase is an enzyme that directs the precursors of advanced glycation end products (AGEs) to pentose phosphate pathway. Benfotiamine administration increases the levels of intracellular thiamine diphosphate, a cofactor necessary for the activation transketolase, resulting in the reduction of tissue level of AGEs. The elevated level of AGEs has been implicated in the induction and progression of diabetes-associated complications. Chronic hyperglycemia accelerates the reaction between glucose and proteins leading to the formation of AGEs, which form irreversible cross-links with many macromolecules such as collagen. In diabetes, AGEs accumulate in tissues at an accelerated rate. Experimental studies have elucidated that binding of AGEs to their specific receptors (RAGE) activates mainly monocytes and endothelial cells and consequently induces various inflammatory events. Moreover, AGEs exaggerate the status of oxidative stress in diabetes that may additionally contribute to functional changes in vascular tone control observed in diabetes. The anti-AGE property of benfotiamine certainly makes it effective for the treatment of diabetic neuropathy, nephropathy and retinopathy. Interestingly, few recent studies demonstrated additional non-AGE-dependent pharmacological actions of benfotiamine. The present review critically analyzed the multifaceted therapeutic potential of benfotiamine. |
| New Member: aanne |
Posted on Wednesday, Sep 1, 2010 - 7:59 pm: Thanks for the response!As per Andym's response, should I be looking into cosopt DrOps to keep eye pressure down if I plan on keeping the horse on a low doesage of topical steroid? Is there any harm in using cosopt DrOps even when the eye pressure is good? As per the comment on benfotiamine, the information actually came off the pub med link supplied. These tests haven't been studied on horses..but I'm curious to know if there could be a link? What is your opinion? Thanks again! Here is the article: Prevention of endotoxin-induced uveitis in rats by benfotiamine, a lipophilic analogue of vitamin B1. Yadav UC, Subramanyam S, Ramana KV. Department of Biochemistry and Molecular Biology, University of Texas Medical Branch, Galveston, Texas 77555-0647, USA. Abstract PURPOSE: To study the amelioration of ocular inflammation in endotoxin-induced uveitis (EIU) in rats by benfotiamine, a lipid-soluble analogue of thiamine. METHODS: EIU in Lewis rats was induced by subcutaneous injection of lipopolysaccharide (LPS) followed by treatment with benfotiamine. The rats were killed 3 or 24 hours after LPS injection, eyes were enucleated, aqueous humor (AqH) was collected, and the number of infiltrating cells, protein concentration, and inflammatory marker levels were determined. Immunohistochemical analysis of eye sections was performed to determine the expression of inducible-nitric oxide synthase (iNOS), cyclooxygenase (Cox)-2, protein kinase C (PKC), and transcription factor NF-kappaB. RESULTS: Infiltrating leukocytes, protein concentrations, and inflammatory cytokines and chemokines were significantly elevated in the AqH of EIU rats compared with control rats, and benfotiamine treatment suppressed these increases. Similarly increased expression of inflammatory markers iNOS and Cox-2 in ciliary body and retinal wall was also significantly inhibited by benfotiamine. The increased phosphorylation of PKC and the activation of NF-kappaB in the ciliary body and in the retinal wall of EIU rat eyes were suppressed by benfotiamine. CONCLUSIONS: These results suggest that benfotiamine suppresses oxidative stress-induced NF-kappaB-dependent inflammatory signaling leading to uveitis. Therefore, benfotiamine could be used as a novel therapeutic agent for the treatment of ocular inflammation, especially uveitis. |
| Moderator: DrO |
Posted on Wednesday, Sep 1, 2010 - 8:37 pm: As far as I know endotoxin (a bacterial cell wall product) induced inflammation also does not play a part in ERU. The first question becomes one of what pathways here may apply to autoimmune inflammation. Then thousands of other questions must be answered to find out if this is a safe effective treatment. I do not see anything that says this is likely to be a useful treatment for ERU, but neither is there anything to say it is not.DrO |
| New Member: aanne |
Posted on Wednesday, Sep 1, 2010 - 9:23 pm: Thanks for clarifying this Dr. O |
| New Member: aanne |
Posted on Tuesday, Sep 7, 2010 - 7:10 pm: Hi again Dr.O.The use of such a potent steroid has me a bit worried about steroid induced glaucoma. How do you rate flurbiprofen in the realm of a potential preventative? He is currently doing well on a once a week dosage. |
| Member: aanne |
Posted on Wednesday, Sep 8, 2010 - 7:37 am: Thought I'd clarify, he is on a once a week dosage of the steroid |
| Moderator: DrO |
Posted on Wednesday, Sep 8, 2010 - 7:47 am: I have not used it as a preventive and do not see any research so I would rate it as experimental. Have you tried dex once every two weeks?DrO |
| Member: aanne |
Posted on Wednesday, Sep 8, 2010 - 5:21 pm: I just had a read over Current therapy in equine medicine By N. Edward Robinson & Kim A. Sprayberry and they suggest that this can lead to corneal melting and perforation. Perhaps I'm best to stick to the steroid, seeing as they both have risks and I know the steroid is working fine.I'll be trying to move towards Dex once every two weeks. Thanks again! |
| Moderator: DrO |
Posted on Thursday, Sep 9, 2010 - 6:24 pm: That is odd Anne, in species it has been used in I find no evidence that flurbiprofen, which has been around for nearly 30 years, is more likely to do harm than steroids. Both have well documented impairment of corneal epithelial healing and steroid potentiation of bacterial and fungul collagenase leading to melting corneal ulcers is legend but I cannot find any evidence in the peer reviewed scientific medical or veterinary literature of "corneal melting" due to this NSAID use.DrO |
| Member: aanne |
Posted on Friday, Sep 10, 2010 - 7:40 am: Perhaps I've misinterpreted what they have written, Here is a screen capture of the Googlebook. It is positive to hear that you have not come across this though in your practice.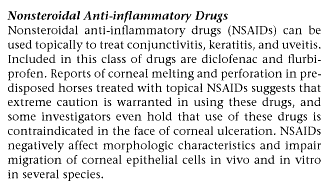
|
| Moderator: DrO |
Posted on Friday, Sep 10, 2010 - 8:00 am: My above comment is not based on clinical experience Ann but research of the scientific and medical literature. I rarely use NSAID opthalmic ointments. If I feel NSAID therapy is indicated for a eye problem I use it systemically to get a little better coverage.The page comment is interesting and I will continue to research this as I do not find scientific evidence to support the idea that NSAID's should be avoided because of a primary severe corneal ulceration. I am uncertain what they mean by "predisposed horses" but if they mean those with preexisting corneal ulcers this caveat would apply equally well with steroid treatment. DrO |
| Member: aanne |
Posted on Sunday, Sep 12, 2010 - 8:58 am: Thanks for your thoughts Dr.O, always appreciated! |
Horseadvice.com
is The Horseman's Advisor
Helping Thousands of Equestrians, Farriers, and Veterinarians Every Day
All rights reserved, © 1997 -
is The Horseman's Advisor
Helping Thousands of Equestrians, Farriers, and Veterinarians Every Day
All rights reserved, © 1997 -
