Overview of Diseases of the Cannon Region of Horses: Metacarpal and Metatarsal Disease
by Robert N. Oglesby DVM
Introduction
Introduction
»
Localization & Diagnosis
»
Diseases of the Cannon
»
More Info & Discussions
The cannon region begins just distal to the knee in the front and hock in the back and travels distally to the fetlock. Within this region you will find the cannon bone, the two splint bones, extensor tendons, flexor tendons, the suspensory, sesamoids, and the check ligament. Though the sesamoid bones might be considered in the distal cannon region because of the standard series of nerve blocks they are, for diagnostic processes, considered part of the ankle (fetlock). With so much anatomy it is not surprising that the cannon region is often associated with lameness and the accurate diagnosis of the soft tissues of the proximal cannon can present a diagnostic challenge.
The cannon bone is called the third metacarpal (Mc3) in the front leg and the third metatarsal (Mt3) in the hind limb. The splint bones are referred to as the second (inside) and forth (outside) metacarpal and metatarsal (abbreviated Mc2, Mc4, Mt2, and Mt4) respectively. This article deals with anatomy of the cannon region and the localization and diagnosis of diseases of the cannon region and cannon bone. Fractures of the cannon bone are covered here while links to other diseases of the cannon region are provided.
Localization & Diagnosis
Introduction
»
Localization & Diagnosis
»
Diseases of the Cannon
»
More Info & Discussions
|
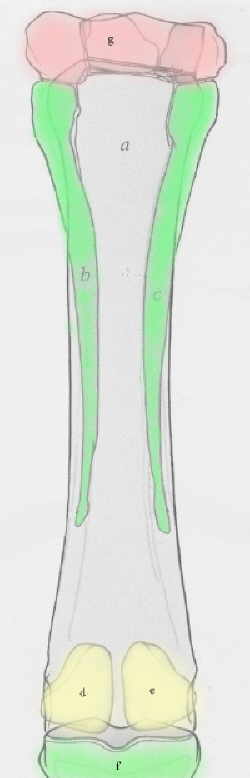
Image: Cannon region as viewed from the back
|
|
|
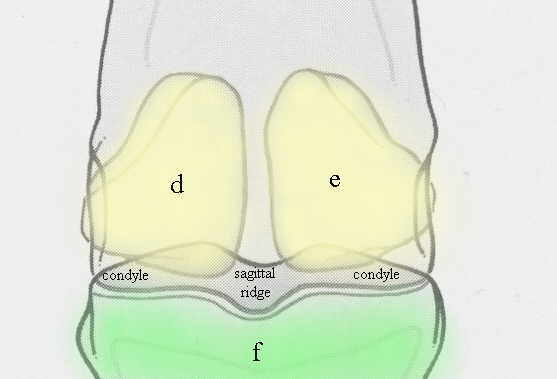
Bottom row of Knee Bones (g), Cannon Bone (a), Splint Bones (green b & c), Sesamoid Bones (yellow d & e), top pastern bone (f), from the back of the cannon.
|
Acute lameness of the cannon is generally found by careful examination. There are no overlying muscles so direct examination and palpation can be done on most of the structures. The one exception would be the suspensory and check ligament in the back which has the flexor tendons overlying them. When a physical exam does not reveal a cause of lameness, the cannon area becomes suspect when the structures below it are ruled out with a low volar four point or ring block and lameness still persists. If a second careful exam of the cannon region still does not reveal the source of lameness nerve blocks to rule out the structures of the cannon region are indicated unless a fracture is suspected. Blocking a nondisplaced fracture can result in the horse becoming fully weight bearing on the lame leg and displace the fracture. If a fracture is suspected radiographs would be the next best step.
Regional Anesthesia of the Cannon
Nerve blocks to the cannon region are fairly easy with a thorough understanding of the anatomy of the two palmar nerves and two palmar metacarpal(tarsal) nerves but beyond the scope of this article. This is callled a high four-point cannon block and effects all the structures in the back of the cannon. There is one fly in the ointment with interpreting this block. Often with this block the two distal joints of the knee are blocked, so lameness originating from these joints may be incorrectly attributed to structures in the cannon. There are several ways to avoid this confusion with the focus should be on a specific diagnosis. The blocks may be the only way to localize the source of the lameness, but should be followed up with diagnostic imaging to locate a lesion. If lameness remains undiagnosed despite radiographs and ultrasound, the knee should then become suspect. By specifically blocking the knee joints
To block the front (anterior) structures and therefore the whole cannon area requires a ring block across the front and sides of the cannon in conjunction with the high 4-point cannon block.
Diagnosis
Once the lameness is positively localized to the region of the cannon diagnosis is usually accomplished with diagnostic imaging particularly radiography and ultrasound. Caution should be exercised by those who are not intimately familiar with the ultrasonographic appearance of the soft tissues of the posterior cannon. It is easy to confuse normal anatomical variation and artifacts created by the improper imaging with real lesions.
Diseases of the Cannon Region
Introduction
»
Localization & Diagnosis
»
Diseases of the Cannon
»
More Info & Discussions
[wcm_restrict]
Considering the size of the horse the cannon bone is a relatively small diameter bone to support the weight of the horse. Also important to note is that though the cannon's anatomy is very similar in the front and back legs that the front cannon works much harder because the horse has more weight on the front legs.
Fractures of the Cannon Bone Shaft (Diaphysis)
It is not surprising that complete fractures of the cannon bone is not uncommon. The fracture can be from simply loading stress during exercise or traumatic as might happen from a kick from another horse. Complete fractures of the cannon are easily diagnosed from the swelling and dislocated appearance of the distal segment. The horse will be completely non-weight bearing and often there is remarkable soft tissue trauma around the fracture site. When there is remarkable destruction of the surrounding tissues, including the arteries and nerves surgery is not an option. In other cases adequate stabilization to move the horse safely to a surgical facility is difficult and often fail. The prognosis for successful surgery is poor in the full size adult horse (greater than 320 kg or 700 lbs) even under good conditions. However smaller horses and foals have a much better prognosis if infection does not become a complication.
The first challenge is to get the horse to a surgical facility without further soft tissue damage. A well constructed splinted Robert Jones bandage can usually be attempted and often the best choice. Pins and plates are required to achieve adequate stability for such a fracture to heal.
Condylar Fracture
Condylar fractures of the distal splint are usually a bit more stable and can be moved with splinting. Displaced condylar fractures require screwing while non-displaced condylar fractures of the hind cannon (metatarsus) have been treated with casting in the standing horse.
|
More Information on Treatment of Medial Condylar Fractures
Vet Rec. 2008 May 3;162(18):586-9.
Treatment of medial condylar fractures of the third metatarsus in three horses with fibreglass casts under standing neuroleptanalgesia.
Lloyd D, Johanson C, Phillips TJ.
Liphook Equine Hospital, Forest Mere, Liphook, Hampshire gu30 7jg.
Minimally displaced condylar fractures propagating into the third metatarsal diaphysis were treated conservatively in one thoroughbred and two Arabian racehorses. In each case a neuroleptanalgesic protocol provided adequate pain relief for a rigid fibreglass cast to be applied in a weight-bearing position. The fractures healed completely and the three horses recovered uneventfully. Two of them returned successfully to racing and the third was used for breeding.
|
Other Diseases of the Cannon Region
Either physical exam or a successful block of the cannon, radiographs of the cannon and splint, ultrasound of the suspensory, check ligament, and flexor tendons should lead one to one of the following structures:
-
Splint bone disease,
...more
-
Suspensory ligament desmitis,
...more.
-
Check ligament desmitis,
...more.
-
Flexor tendonitis,
...more.
-
Bucked Shins or Fissure Fractures on the Cannon,
...more.
For More Information on this Topic:
Introduction
»
Localization & Diagnosis
»
Diseases of the Cannon
»
More Info & Discussions
Search the National Library of Medicine for all the summaries on this topic. Just push the button the search fields have been already filled in:
[/wcm_restrict][wcm_nonmember] [text-blocks id="article-ender-join"][/wcm_nonmember]
 .
.